极速赛车一分钟168开奖官网 极速1分钟一68记录 Smarter subscription experiences
Powering your growth and retention strategy
Drive more revenue from your subscription strategy with meaningful insights, dynamic subscriber experiences, and a subscription core trusted by over 20,000 brands. We don't just help you sell products, we help you build buyer routines that last.




The #1 most
trusted subscription platform
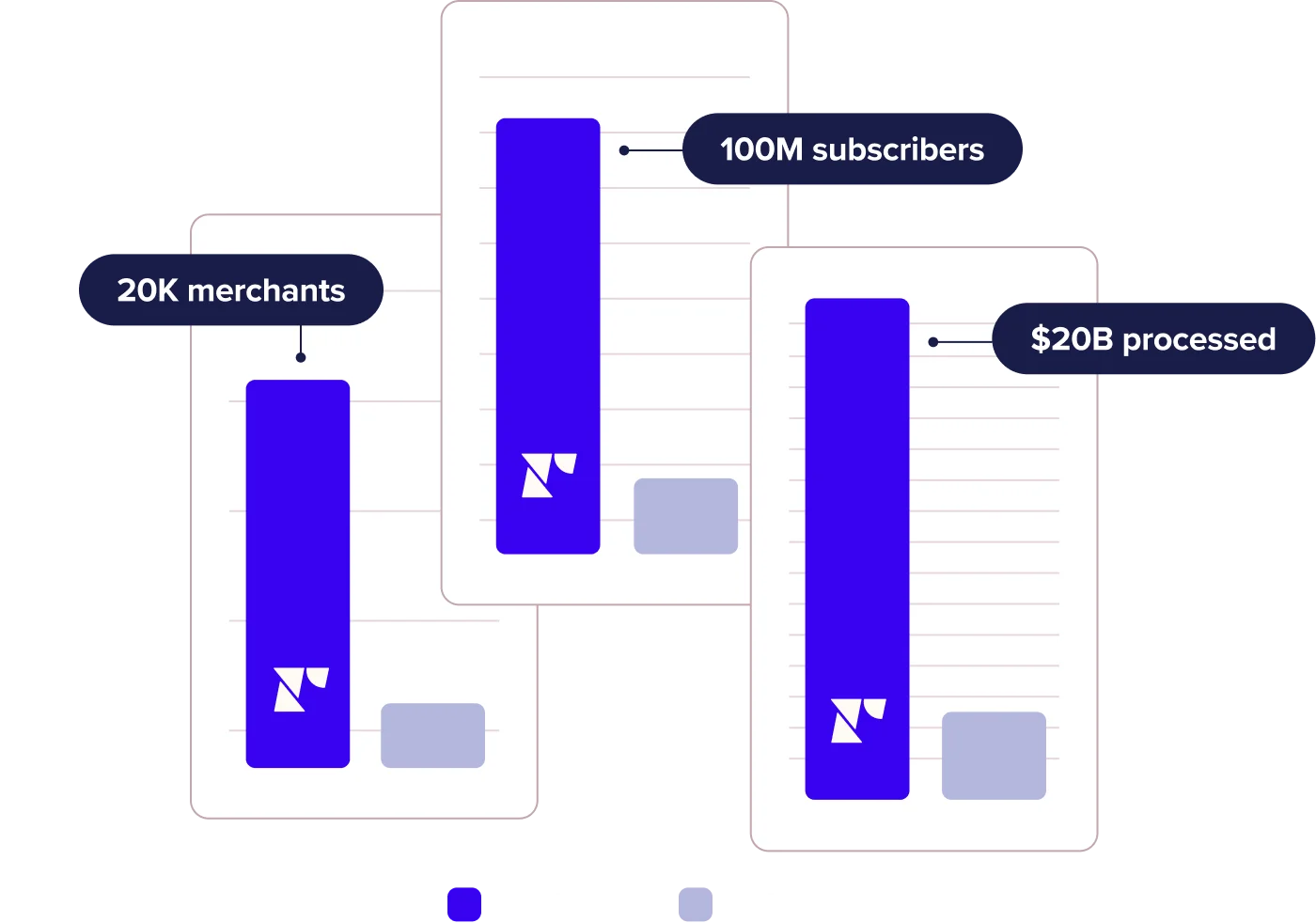
20,000
Brands served
100M
Subscribers
$20B+
Processed

The world's best brands are 极速赛车1分钟计划开奖记录+168开奖官网查询结果 powered by routine, and the world's best routines are powered by Recharge
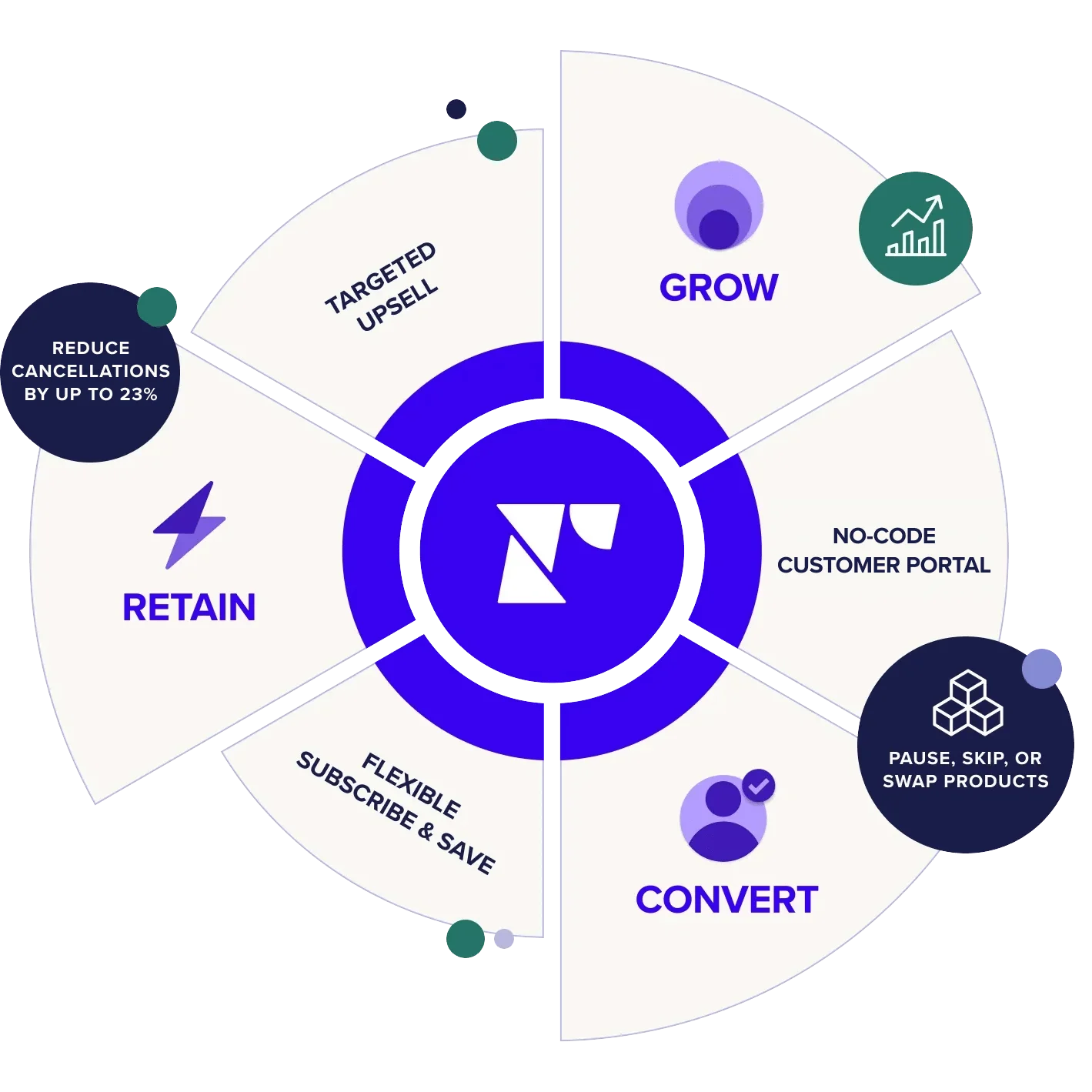
Grow your business with Recharge
Trusted
Subscription management
Go beyond the basics. Easy subscription management, no-code customer portals, dynamic bundles, tiered discounts—Recharge powers it all.
 Learn more
Learn more
Robust
Analytics & insights
Learn, iterate, grow. Use Recharge's intelligent insights to monitor your business's performance and optimize results.
 Learn more
Learn more
Dynamic
Subscription experiences
Deliver dynamic experiences. Craft personalized experiences at every touchpoint. Offer free gifts or discounts on upcoming orders, save cancellations with personalized retention offers, and more.
 Learn more
Learn more
168极速赛车官方官网开奖记录|历史数据结果-开奖历史1分钟记录查询 Your all-in-one solution for retention and growth
We're putting 100 million subscribers to work—for you
The Recharge platform supports over 100 million subscribers. What does that mean for you?
It means that 100 million subscribers inform our product decisions, the tactics we recommend to you, and the insights we empower your business with.
Out-of-the-box functionality & robust customization
Start processing revenue immediately with robust no-code options—and endlessly customize as you scale with our API.
Developer Hub Recharge API Product documentation
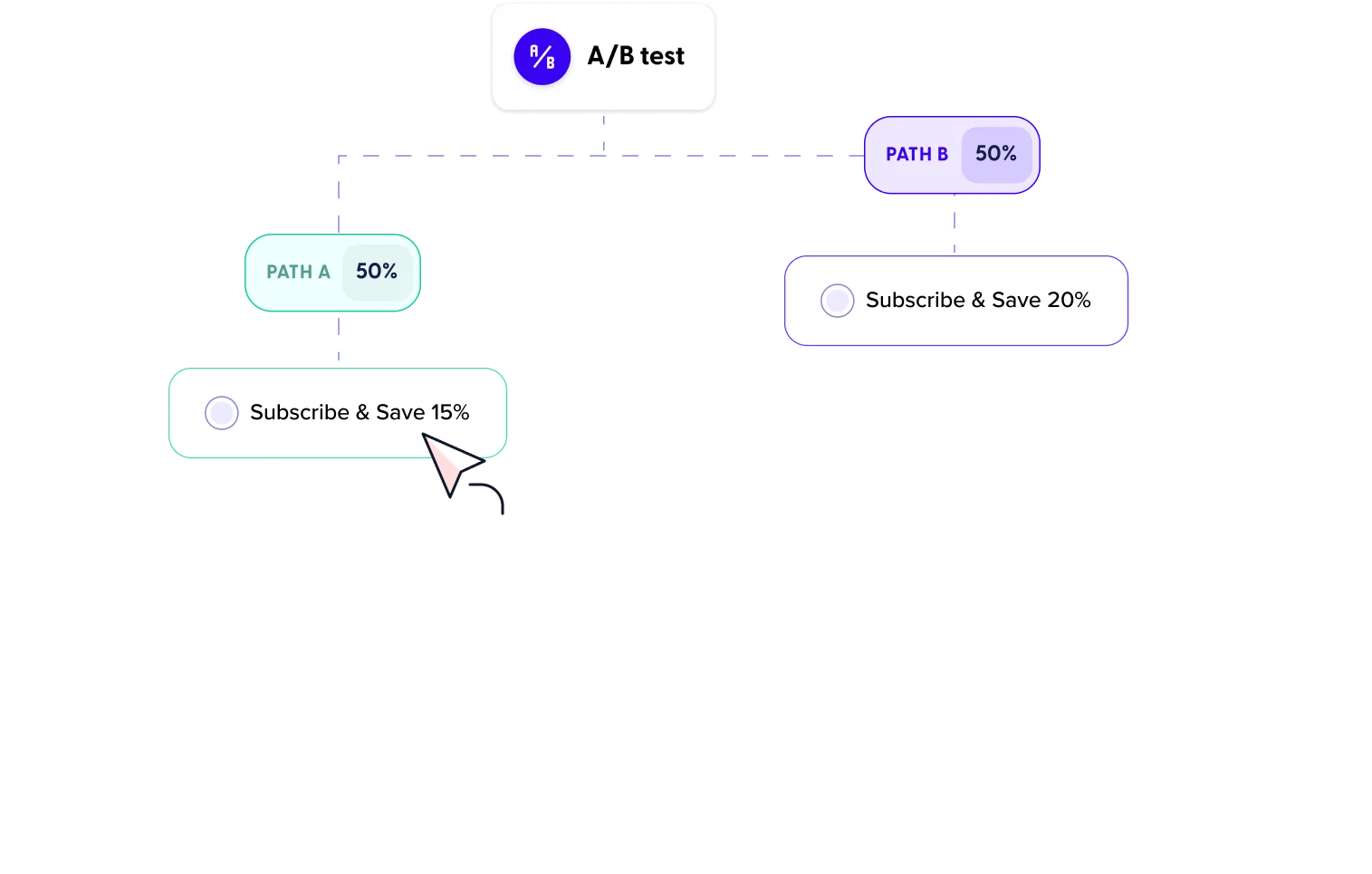
Iterate & test
All the functionality you need to increase LTV and all the flexibility you need to quickly iterate and test your retention and growth programs.
Subscription services在线168赛车直播结果一分钟记录 正规开奖历史 Built to scale with you
The best suite of tools to start and customize your subscription strategy—all based on your unique business goals.
Get in touch
The #1 most trusted subscription platform
Subscriptions are complex. It's a whole process—a process we've completed over 20,000 times. We're experts at scoping your needs, tackling technical hurdles, and scaling as you grow.
$300M+
In GMV migrated from other subscription platforms in 2023
<2 hours
Average ticket initial response time
<1 minute
Average chat wait time
The Recharge ecosystem
Leverage the largest network of tech and agency partners to seamlessly connect all areas of your business and perfect your entire subscription lifecycle.
Agency partners Technology partners